In a 2010 analysis of NSCLC diagnoses in the National Cancer Database, 26% of lung cancers were diagnosed at Stage I, 28% were diagnosed at Stage III when resection is often impossible, and 38% were diagnosed at Stage IV [18]. Similarly, the latest Surveillance, Epidemiology, and End Results program statistics report that 16% of lung cancers are diagnosed as a localized diseases versus 57% as a distant or metastatic diseases [19]. In recent years, there has been a slight trend of increased incidence of Stage I at diagnosis, which could be attributed to the improved evaluation of incidental nodules (with approximately 1.5 million such findings being made annually outside of the lung cancer screening setting) [5].
The reason for a late diagnosis is that lung cancer typically doesn't have signs and symptoms in its earliest stages, and once they appear, they are mainly non-specific and may include:
These symptoms are not lung cancer-specific and could also be characteristic of other diseases. Most frequently, lung cancer is misdiagnosed as COPD, asthma, gastric reflux, lung abscesses, tuberculosis, and bronchial pneumonia. Another group of clinical symptoms appears when the disease is advanced and, to a significant extent, represents organs involved in the pathological process: bone pain, headaches, and other symptoms related to the central nervous system (CNS).
Radiology assessments sometimes are also not conclusive. A variety of fungal pulmonary infections can produce radiologic findings that mimic lung cancers [20]. The modality of a radiological evaluation matters as about 90% of presumed mistakes in pulmonary tumor diagnosis occurred on chest radiography, only 5% on CT examinations, and the remaining 5% on other imaging studies [21]. The reasons for a misdiagnosis on chest radiography, and less frequently on CT scans, can include observer error (scanning, recognition, and decision-making error), specific characteristics of the undetected lesion (size, conspicuity, and location), and technical inaccuracies [22]. The primary need in lung cancer management is an early diagnosis, preferably of asymptomatic or minimally symptomatic patients. This is typically accomplished with screening protocols. Large pre-defined groups of people undergo diagnostic procedures that are easy and inexpensive to apply, and which provide an accurate and specific result. There are two major categories of screening procedures for lung cancer: radiology scanning techniques and biomarkers.
Several groups, including ASCO, provide recommendations for lung cancer screening based on age and smoking history. In 2021, the US Preventive Services Task Force issued recommendations for annual lung cancer screening with low-dose computed tomography (LDCT) in adults aged 50 to 80 years who have a 20 pack-year smoking history (equivalent to the number of packs smoked per day multiplied by the number of years the person has smoked) and currently smoke or have quit within the past 15 years [23]. The National Lung Screening Trial demonstrated a 20% relative reduction in lung cancer mortality [24].
Once lung cancer is suspected, the diagnostic evaluation includes three simultaneous steps: tissue diagnosis, staging, and functional evaluation.
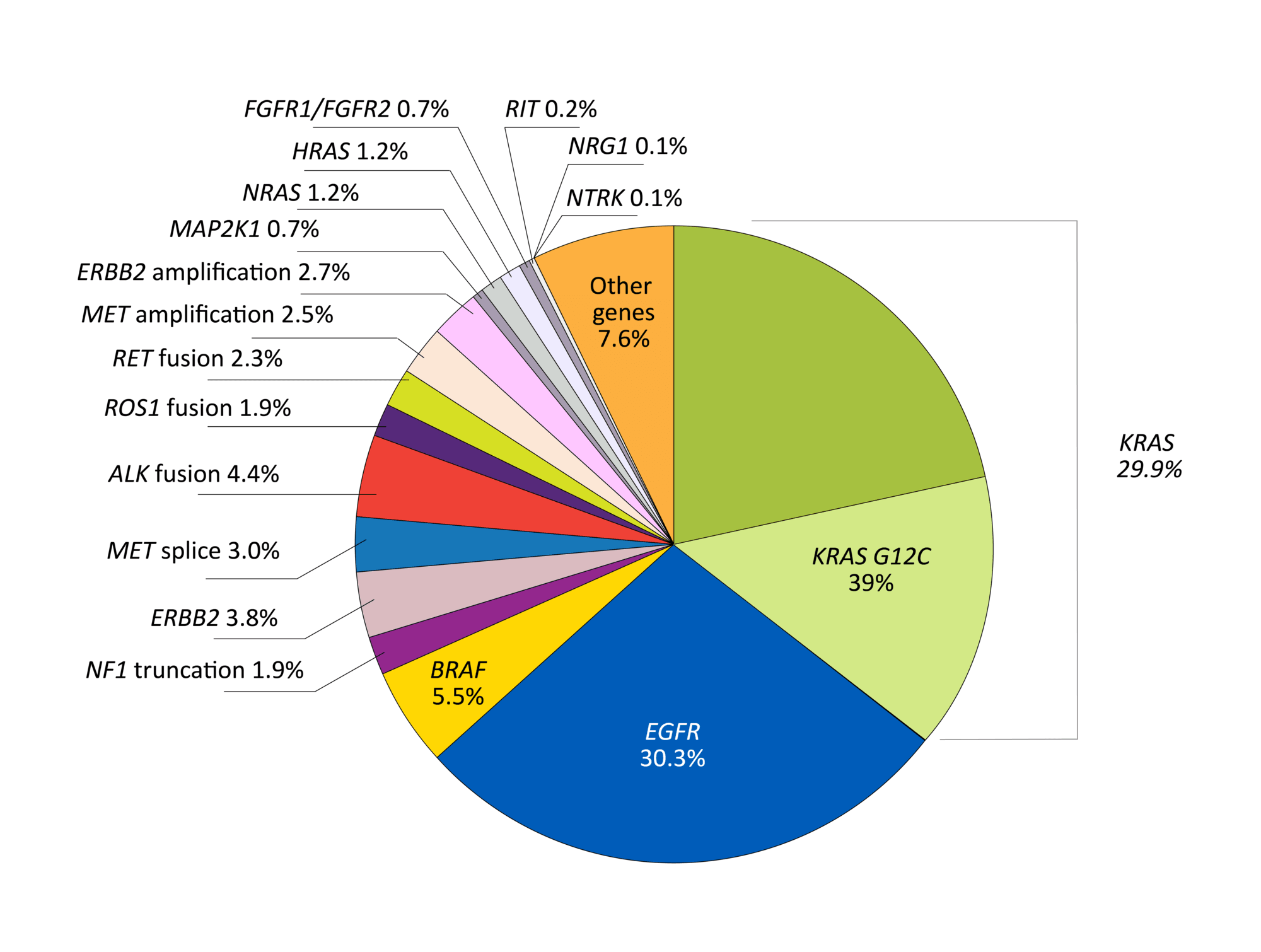
The exact diagnosis of lung cancer is based on a histological method that subdivides lung cancer into two major groups: SCLC and NSCLC. This dichotomic classification existed for decades and was sufficient with the existing treatment option of platinum doublets. In 2004, an epidermal growth factor receptor (EGFR) and HER2 mutations were discovered in NSCLC patients, leading to the introduction of specific targeted drugs. With the further development of treatment options and diagnostic improvements, it is now necessary to diagnose the disease histologically and molecularly characterize it (Fig. 4) [25].
Biomarkers may be predictive (or actionable), with a corresponding targeted therapy; or prognostic to help understand patients’ survival perspectives.
The current diagnostic standard requires a minimum set of actionable mutations to be tested: ALK (anaplastic lymphoma kinase) rearrangements, BRAF (B-raf proto-oncogene), EGFR (epithelial growth factor receptor), mesenchymal-epithelial transition exon 14 skipping, NTRK1/2/3 (neurotrophic tyrosine receptor kinases) gene fusions, RET (rearranged during transfection) rearrangements, and ROS1 (ROS proto-oncogene 1) rearrangements [26].
To be able to do this, adequate tissue sampling is required. Several techniques are currently used, including endoscopic ultrasound-guided fine-needle aspiration, radial EBUS, navigational bronchoscopy or mediastinoscopy, transthoracic needle aspiration, and surgical excision. However, it may not be feasible to get an adequate amount of the tissue, or a biopsy may not be possible at all. There is also a frequent need for repeated tissue biopsies to monitor the evolution of the tumor, which is burdensome and not feasible for every patient. Because of this, circulating biomarkers—so-called liquid biopsy—have gained significant attention in recent years.
Circulating tumor cells and circulating cell-free DNA (cfDNA) are the most studied liquid biopsy-derived biomarkers, but many others are also under investigation. Cancer patients have higher levels of cfDNA than healthy individuals and, since the tumor volume correlates with cell turnover and death, circulating tumor DNA (ctDNA) concentration increases with tumor size. Plasma ctDNA analysis may identify molecular alterations in patients when sufficient tissue is not available [27].
The approach to biopsy a technically accessible disease site poses another question of whether samples from the primary tumor or metastatic sites are equally suitable for determining patient eligibility for targeted therapies. This question is still under debate. There was a substantial concordance between primary and metastatic tumor sites for some mutations, such as EGFR, KRAS, and BRAF mutations. At the same time, some level of discordance was seen in most published studies attributing a key role to mutation testing methodologies [28].
For EGFR mutations, a good overall concordance between primary lung tumor and distant metastases is common. Compared with CNS and lung/pleural metastases, higher discordance rates are observed in bone metastases [29]. A potential discordance in mutation status between the primary lung lesion and metastatic sites may be responsible for some share of anti-cancer treatment inefficacy. Future research is necessary to assess the impact of mutation discordance on treatment efficacy and survival.
Within the past several years, the improvement of molecular biology techniques contributed to the identification of specific mutated oncogenes in NSCLC for which treatments have either become commercially available or are under investigation, leading to a paradigm shift in the treatment of NSCLC. Therefore, appropriate tumor sampling is essential not only for histological subtyping but also for accurate tissue genotyping.
There are several popular methods for molecular profiling: real-time polymerase chain reaction, next-generation sequencing (NGS), Sanger sequencing, fluorescence in situ hybridization, and immunohistochemistry (IHC). These methods are not equal in terms of the assay’s sensitivity and the quality and quantity of the tumor sample used. Routinely, the first step remains a pathological diagnosis and IHC analysis of such biomarkers as thyroid transcription factor-1 (TTF-1) and Napsin-A, which helps to distinguish between adenocarcinoma and squamous cell carcinoma as well as determine that the tumor under question is lung primary. In parallel, programmed death-ligand 1 (PD-L1), anaplastic lymphoma kinase (ALK), or ROS1 are evaluated. For molecular testing, a broad panel-based approach is recommended, and it typically utilizes NGS assays that allow the evaluation of all actionable biomarkers with just one test. When extrapolating the above to the clinical trials environment, it is critical to use approved testing techniques, especially with targeted therapy. Across Europe, there is considerable variability in the uptake of biomarker testing technologies. For example, the proportion of patients with advanced nonsquamous NSCLC who received a molecular test varied between 65% and 85% across Germany, Italy, and Spain [30]. Along with the testing availability, other considerations include international recognition of the test, whether it is centrally or locally run, and turnaround time.
© PSI, 1995 – 2021. All rights reserved
Fig.4 Prevalence of oncogenic mutations in NSCLC. From: Skoulidis F, Heymach J, 2019 [25]