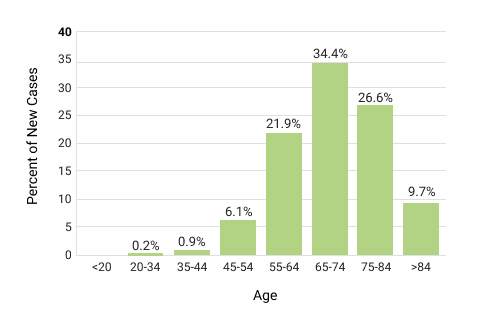
Morbidity data from the population-based US Cancer Statistics database (2010-2017) showed that 53% of patient deaths during this time were male and 67% had an age of ≥ 67 years [5], suggesting that male gender and advanced age are risk factors for lung cancer. The most frequently affected age cohort is 65-74 years with a median age at diagnosis of 71 years (Fig. 3) [2].
Other factors have different power and distribution over the globe, including tobacco smoking; previous radiation, including radon exposure; air pollution; and genetics.
Fig.3. Percent of new cases by age group (all races, all sexes). From: National Cancer Institute: Cancer Stat Facts: Lung and bronchus cancer // https://seer.cancer.gov/statfacts/html/lungb.html
© PSI, 1995 – 2021. All rights reserved
Lung cancer is among those malignant diseases in which the role of smoking has been not only suspected but proven. Up to 90% of lung cancer deaths have been linked to cigarette smoking. Secondhand smoke (also known as “environmental tobacco smoke” or “passive smoke”) is also generally considered an established risk factor for the development of lung cancer. However, some argue that there is no clear link between secondhand smoke and lung cancer development [7].
Chewing tobacco and other smokeless tobacco products are often promoted as safer than cigarettes. Still, there are ongoing discussions in society and medical literature over whether there are any less harmful tobacco-containing products. One of the most popular oral smokeless tobacco products is snus. This substance is usually placed behind the upper lip and is primarily used in Sweden and Norway, being prohibited by legislation in other European Union (EU) countries. Several epidemiological studies have shown either low or minimal (not exceeding the population) risk of lung cancer in snus users [8]. In Sweden, the incidence of lung cancer was 40.1 per 100.000 population—the lowest among European countries [9]. In parallel, death rates due to lung cancer in Sweden are also lower than in most of the European countries.
These data do not advocate the use of smokeless tobacco products in general, as they still increase the risk of cancer of the oral cavity, pharynx, esophagus, and possibly the pancreas [10]. However, it clearly shows that smoking tobacco is the leading harmful tobacco product related to lung cancer, but it is not the only risk factor for the disease. Not all smokers, or even all heavy smokers, get lung cancer. Approximately 10% to 15% of lung cancer cases in the United States occur in never-smokers, and the proportion of never-smoker NSCLC patients increased from 8% in the years 1990-1995 to 15% in 2011-2013 [11], indicating that other factors may play a role in NSCLC development.
Radon is one of the major risk factors for lung cancer. In 2019, residential radon exposure alone was estimated to have caused 84,000 deaths by lung cancer globally; in some countries, it is among the leading causes of lung cancer [12].
The rate of lung cancer deaths attributable to air pollution varies widely between countries. Serbia, Montenegro, Bosnia, China, Mongolia, and Poland are among the worst affected, with a strong association between deaths from lung cancer and the proportion of national energy produced from coal [13].
Other environmental or external risk factors include asbestos, radioactive ores such as uranium, inhaled chemicals (arsenic, silica, vinyl chloride, and nickel and chrome compounds), diesel exhaust, arsenic in drinking water, and radiation therapy to the lungs.
Familial cancer is characterized by gene mutations in two or more first‑degree relatives diagnosed with the same type of cancer. Approximately 8% of lung cancers are inherited or occur because of a genetic predisposition [14].
Pre-morbid conditions or concomitant diseases also matter, particularly those that influence the respiratory system, such as Chronic Obstructive Pulmonary Disease (COPD). Both COPD and lung cancer are linked to tobacco smoking.
COPD is an independent risk factor for lung carcinoma, particularly for squamous cell carcinoma, and lung cancer is up to five times more likely to occur in smokers with airflow obstruction than those with normal lung function [15].
In patients with COPD, the structural changes in the lungs and airflow limitations caused by the inflammation and deregulation of the inflammatory repair response and altered signaling via the epidermal growth factor receptor may lead to the development of lung cancer. Other comorbidities that influence the survival of lung cancer patients include diabetes and tuberculosis [16]. Not all comorbidities or simply the number of concomitant diseases will directly influence the prognosis. Patients with concurrent comorbidities can be included in clinical trials for many aggressive tumors without significant concern about masking any survival benefit owing to the intervention [17]. However, the number and severity of comorbidities may influence the patient’s performance status (often part of the inclusion criteria) and predispose such patients to more frequent adverse events and serious adverse events with the potential for treatment dose modifications or interruptions. In turn, these can decrease the treatment dose density and intensity and potentially lower treatment efficacy.
Approximately 8% of lung cancers are inherited or occur because of a genetic predisposition.