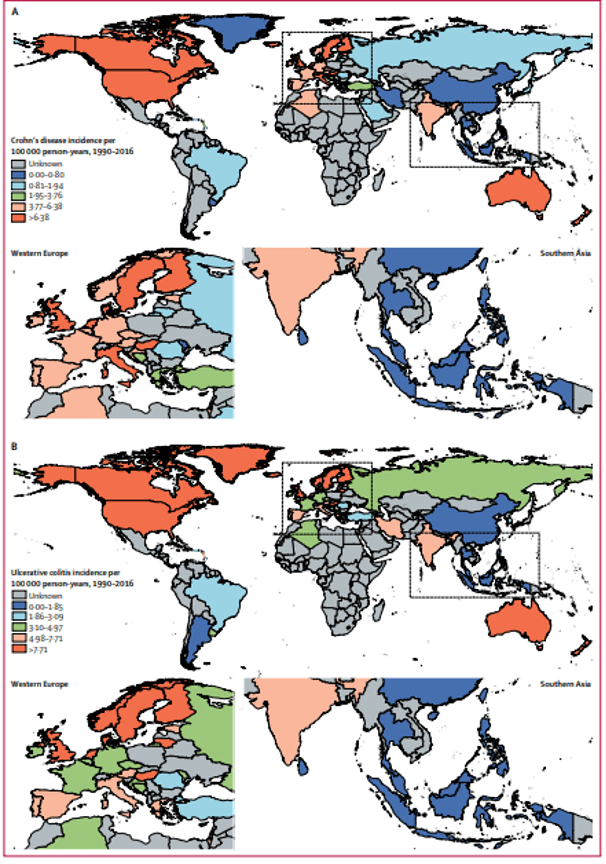
The highest reported prevalence rates for UC were in Norway (505 per 100,000 population) and the U.S. (286 per 100,000 population) while CD was most prevalent in Germany (322 per 100,000 population) and Canada (319 per 100,000 population).1 Cohort studies from Asia, Africa, and South America have consistently described the rising incidence of IBD in countries outside the Western world (Fig 1). The pattern of IBD in the East resembles that of the West, and though differences still exist (particularly in environmental factors presumably provoking development of IBD, e.g. industrialization and dietary changes), a balance between East and West is approaching.2
Overall trends in IBD incidence show a steady increase year over year. The US alone had 1.8 million patients with IBD in 1999 and 3.1 million in 2015.3 A forecast of the global burden of IBD between 2015 and 2025 predicted exponential growth of the number of patients, due to increased rates of diagnosis and low mortality, and trends currently remain consistent.4
IBD can occur at any age, but the most frequent age distribution of new cases is described as a “bell-curve” with the first and major peak in people at 30-40 years and the second, smaller peak at 60-70 years.5 Approximately 25% of IBD patients are younger than 18 years.6 Rates of pediatric-onset IBD continue to rise around the world and data are emerging from regions where it was not previously reported.7
Between 1999 and 2017, the overall hospitalization rate for CD and UC decreased among older adults, with a sharper decline in the hospitalization rate for UC.8 At the same time, rising costs of medications contributed to making the annual mean health care costs for patients with IBD over three times higher than patients without IBD (approximately $23,000 versus $7,000).9 On the country level, for example in the US, the annual health care spending on IBD increased from $6.4 billion in 1996 to $25.4 billion in 2016.10